
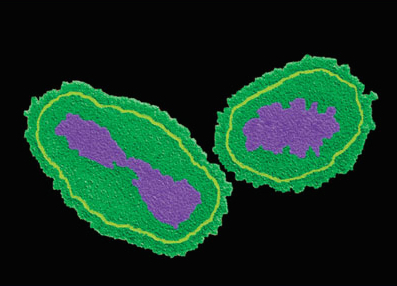
If we mapped out the family tree of poxviruses, then vaccinia virus (the causative agent of cowpox) and variola virus (the causative agent of smallpox) would probably be sisters. Or at the very least, cousins. This close heritage allows the relatively benign vaccinia virus to confer variola virus-protective immune responses in vaccinated individuals.
A safely attenuated version of vaccinia virus, called modified vaccinia ankara (MVA), lies at the heart of the modern smallpox vaccine. Learning more about the biology of MVA helps us to understand why this vaccine is so great at protecting us from smallpox.
Scientists at Memorial Sloan-Kettering Cancer Centre in the USA have now discovered how MVA triggers innate immune responses during infection. They found that MVA DNA is detected by the immune sensors cGAS and STING, which activate secretion of type I interferons in a very specialised immune cell population – the conventional dendritic cells (cDCs).
Yet vaccinia doesn’t passively accept the activation of these immune reactions that are designed to shut it down. Instead, it expresses a variety of virulence factors that inhibit these immune pathways and allow it to survive. This information could be used to improve the utility of MVA as a vaccine against other diseases, like cancer.
Image credit: Weltzin et al 2003
Repost from the Stojdl Lab blog.


 After applying this algorithm across archived tumour biopsies from 511 patients, the team identified genetic alterations in their 121 target genes in 80% of patients. In a mini study to test the clinical utility of this approach, they generated personalised tumour genetic profiles for 16 cancer patients within 16 days, and used this information to siphon patients with certain exome mutations into matched clinical trials testing genetically complementary therapies. For example, one patient with metastatic lung adenocarcinoma exhibiting a KRAS-activating mutation (A146V) was enrolled in a phase I clinical trial of the CDK4 inhibitor, LY2835219 (preclinical data suggests a lethal relationship between activated KRAS and CDK4). This led to stable disease; the patient’s best and only clinical response to any cancer therapy.
After applying this algorithm across archived tumour biopsies from 511 patients, the team identified genetic alterations in their 121 target genes in 80% of patients. In a mini study to test the clinical utility of this approach, they generated personalised tumour genetic profiles for 16 cancer patients within 16 days, and used this information to siphon patients with certain exome mutations into matched clinical trials testing genetically complementary therapies. For example, one patient with metastatic lung adenocarcinoma exhibiting a KRAS-activating mutation (A146V) was enrolled in a phase I clinical trial of the CDK4 inhibitor, LY2835219 (preclinical data suggests a lethal relationship between activated KRAS and CDK4). This led to stable disease; the patient’s best and only clinical response to any cancer therapy.



